
Our latest large study about excess mortality during Covid released today: Demonstration that there was no contagion or spread, only unnecessary harm
High-resolution geotemporal analysis for the Northern Hemisphere (USA and Europe)



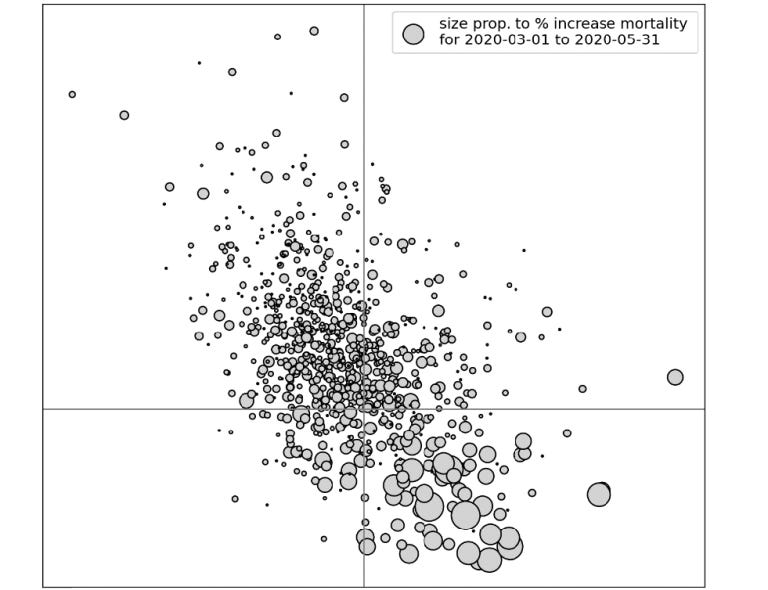
The report is 400+ pages, with hundreds of graphs.
This full version conveniently has an in-text index and an electronic index (left bar in PDF): https://correlation-canada.org/constraints-on-hypothesis-of-disease-spread-during-Covid/
The report was first published at preprints.org.
Below are the Abstract and Conclusion sections.
Constraints from geotemporal evolution of all-cause mortality on the hypothesis of disease spread during Covid
Joseph Hickey,1,2,* PhD ; Denis G. Rancourt,1 PhD ; Christian Linard,1,2 PhD
1 Correlation Research in the Public Interest (correlation-canada.org)
2 Université du Québec à Trois-Rivières (uqtr.ca/PagePerso/Christian.Linard)
* joseph.hickey@alumni.ucalgary.ca
June 13, 2025
Abstract
Large peaks of excess all-cause mortality occurred immediately following the World Health Organization (WHO)’s March 11, 2020 COVID-19 pandemic declaration, in March-May 2020, in several jurisdictions in the Northern Hemisphere. The said large excess-mortality peaks are usually assumed to be due to a novel and virulent virus (SARS-CoV-2) that spreads by person-to-person contact, and are often referred to as resulting from the so-called first wave of infections. We tested the presumption of this viral spread paradigm using high-resolution spatial and temporal variations of all-cause mortality in Europe and the USA.
We studied excess all-cause mortality for subnational regions in the USA (states and counties) and Europe (NUTS statistical regions at levels 0-3) during March-May 2020, which we call the “first-peak period”, and also during June-September 2020, which we call the “summer-peak period”.
The data reveal several definitive features that are incompatible with the viral spread hypothesis (in comparison with qualified predictions of the leading spatiotemporal epidemic models):
· Geographic heterogeneity of first-peak period excess mortality: There was a high degree of geographic heterogeneity in excess mortality in the USA and Europe, with a handful of geographic regions having essentially synchronous (within weeks of each other) large peaks of first-peak period excess mortality (“F-peaks”) and all other regions having low or negligible excess mortality in the said first-peak period. This includes vastly different F-peak sizes (up to a factor of 10 or more) for subnational regions on either side of an international border, such as Germany’s NUTS1 regions on its western border (small F-peaks) compared to the NUTS1 regions on the other side of the international border in the Netherlands, Belgium and France (large F-peaks), despite significant documented cross-border traffic volumes between the regions.
· Temporal synchrony of first-peak period excess mortality: F-peaks for USA states and European countries were almost all positioned within three or four weeks of one another and never earlier than the week of the WHO’s pandemic declaration. For a given large-F-peak European country, the F-peaks for all subnational regions rose and fell in lockstep synchrony but showed large variation in peak height and total integrated excess mortality. A similar result was seen for the counties of large-F-peak USA states.
· Large differences in first-peak period excess mortality for comparable cities with large airports in the same countries: We compare mortality results for Rome vs Milan in Italy, and Los Angeles and San Francisco vs New York City in the USA, and show that there was a dramatic difference in first-peak period excess mortality between the compared cities, despite their having similar demographics, health care systems, and international air travel traffic, including from China and East Asia.
We also examined data concerning the location of death (whether in hospital, at home, in a nursing home, etc.) and socioeconomic vulnerability (poverty, minority status, crowded living conditions, etc.) at high geographic resolutions, which support an alternative hypothesis that excess mortality in jurisdictions with large F-peaks was caused by the application of dangerous medical treatments (in particular, invasive mechanical ventilation and pharmaceutical treatments) and pneumonia induced by biological stress due to treatment and lockdown measures.
Exceptionally large F-peaks occurred in areas with large publicly-funded hospitals serving poor or socioeconomically frail communities, in regions where poor neighbourhoods are situated in proximity to wealthy neighbourhoods, such as the case of The Bronx in New York City, and the boroughs of Brent and Westminster in London, UK.
Taken together, our study represents strong evidence that the patterns of excess mortality observed for the USA and Europe in March-May 2020 could not have been caused by a spreading respiratory virus, and instead were due to the medical and government interventions that were applied and mostly killed elderly and poor individuals.
Conclusion
Using high-resolution all-cause mortality data for Europe and the USA, we have shown that geotemporal mortality patterns during the early months of the declared SARS-CoV-2 pandemic are incompatible with the paradigm of a spreading viral respiratory disease.
It appears that the excess mortality could not have been caused by a viral pandemic. Instead,
· the essential synchrony (within weeks) in mortality hotspots (large “first peaks” or “F‑peaks”) immediately following the WHO’s March 11, 2020 announcement of a pandemic, across countries and states on two continents in the Northern Hemisphere,
· the absence of a single F-peak-like excess mortality event (i.e., rise—peak—fall or rise—plateau) prior to the WHO’s March 11, 2020 declaration of a pandemic,
· the extreme geographical heterogeneity of the magnitude of any excess all-cause mortality as P-score in the time period (“first-peak period”) of the said hotspots,
· the striking differences in the occurrences of hotspots (presence or absence) in entirely comparable large cities in the same countries (Milan vs Rome in Italy; New York City vs Los Angeles and California in the USA),
· the systematic increases in shares of institutional (versus home) deaths in mortality hotspot jurisdictions, and
· the strong correlations to socioeconomic vulnerability of hotspot intensity in high-geographical-resolution sectors within hotspot urban regions,
suggest the alternative hypothesis that first-peak period excess mortality, where it occurs, was of institutional and iatrogenic origin, caused by mistreatment of frail and vulnerable people in hospitals and nursing homes.
In our extensive Discussion (section 4), we compared our results regarding all-cause mortality P‑scores (excess number of deaths divided by expected number of deaths for a time-period, expressed as a percent) with the predictions of large-scale spatial epidemic models, and found that the leading models predicted geotemporal infection and mortality patterns that are of a qualitatively different character than the observed P-scores. The observed geotemporally resolved P-scores are incompatible with the predictions of large-scale spatial epidemic models. We argued (sections 4.1.2, 4.2, and 4.3) that the known insuficiencies of the said models can only bolster our conclusion. Basically, spread must produce spread and pandemic contagiousness must produce widespread penetration, whereas we observe synchrony and both largescale and small-scale patchiness.
The empirical results presented herein provide hard constraints on any and all other contagious spread models. Any model or explanation regarding the cause of excess all-cause mortality during March-May 2020 must comply with our empirical results.
Our analysis of correlations between excess mortality P-scores and socioeconomic variables at the resolution of boroughs in New York City and London, UK exposes the striking observation that the most extreme first-peak period excess mortality occurred in neighbourhoods in which very poor or socioeconomically vulnerable people live in close proximity to very wealthy people. This was examined in some detail for New York City borough of The Bronx, and the London boroughs of Brent and Westminster, in sections 4.5.4 and 4.5.5. We propose that this may be due to the existence of large “safety-net” hospital complexes in poor neighbourhoods that are funded in large part by philanthropy of wealthy residents who live in nearby areas of the same city, such as within the same borough (Brent and Westminster) or in a neighbouring borough (Manhattan, which is adjacent to The Bronx). The same kind of circumstances were present in the Milan area of Italy, in which large hospitals recruited into turbo-charged ICU facilities from large catchments of poor and vulnerable clients. If you were poor, it appears it was especially dangerous to live near well-meaning wealthy social classes offering large-hospital facilities.
This means that the paradigm that a spreading viral respiratory disease caused the excess mortality during Covid is false. The said paradigm is disproved by empirical observations of high-resolution (weekly-monthly, county-region) geotemporal variations of age and frailty adusted excess mortality (P-score) on two continents in the Northern Hemisphere.
Instead, the excess mortality appears to be entirely iatrogenic and induced by the imposed so-called pandemic response.
Therefore, if this is correct, any comments about circulating viruses or variants (e.g., based on PCR or antibody tests of bodily fluids), whether true or false, are irrelevant to the excess mortality.
It is time to acknowledge that a paradigm shift may be necessary, and to adjust epidemiological thinking accordingly.
All the content on my substack is completely free, never behind a paywall or registration-wall.
Nonetheless, please consider becoming a paid subscriber to support our work, if you can.
 | A guest post by
|
 | A guest post by
|
See this outstanding review and explanation of our report: https://unbekoming.substack.com/p/hospitals-not-viruses-what-really
Nuremberg level crimes.